
About Health Inequalities
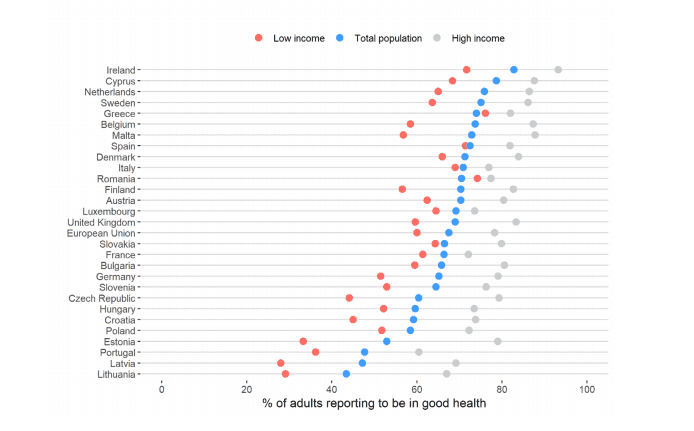 Disparities in self-reported health by income (Forster, T., Kentikelenis, A., Bambra, C.; Health Inequalities in Europe: Setting the Stage for Progressive Policy Action; https://doi.org/10.13140/RG.2.2.20665.21608)
Disparities in self-reported health by income (Forster, T., Kentikelenis, A., Bambra, C.; Health Inequalities in Europe: Setting the Stage for Progressive Policy Action; https://doi.org/10.13140/RG.2.2.20665.21608)

Self-perceived health of the bottom 20% of the poorest population compared to the average population and the top 20% of the richest population. Taken from the EuroHealthNet factsheet on health inequalities.
Health inequalities and COVID-19
 The CHAIN infographic illustrates that COVID-19 is in fact a syndemic pandemic (link)
The CHAIN infographic illustrates that COVID-19 is in fact a syndemic pandemic (link)
It is predicted that the COVID-19 pandemic will lead to economic recession across Europe, which will exacerbate health inequalities. It is becoming increasingly evident that those in lower income groups, and low skilled employment are most likely to catch and die of the disease. The COVID-19 pandemic will exacerbate those pre-existing health inequalities, and have the heaviest impact on the lives of people living in deprivation. The limited data already available (from the UK) suggests that low skilled men have the highest death rate among working age adults. Further research suggest that Black males and females are 4.2 and 4.3 times respectively more likely to die from a COVID-19-related death than White ethnicity males and females. It seems that most fatalities are amongst those with underlying illnesses such as high blood pressure, diabetes and heart or respiratory disease 2Hans Henri P Kluge, *Kremlin Wickramasinghe, Holly L Rippin, Romeu Mendes, David H Peters, Anna Kontsevaya, Joao Breda; Prevention and control of non-communicable diseases in the COVID-19 response; https://doi.org/10.1016/ S0140-6736(20)31067-9 3 Martini N, Piccinni C, Pedrini A, Maggioni A; CoViD-19 and chronic diseases: current knowledge, future steps and the MaCroScopio project; Recenti Prog Med. 2020 Apr;111(4):198-201. doi: 10.1701/3347.33180; https://www.ncbi.nlm.nih.gov/pubmed/32319439 4 Wang B, Li R, Lu Z, Huang Y; Does comorbidity increase the risk of patients with COVID-19: evidence from meta-analysis;Aging (Albany NY). 2020 Apr 8;12(7):6049-6057. doi: 10.18632/aging.103000. Epub 2020 Apr 8.;https://www.ncbi.nlm.nih.gov/pubmed/32267833.
The more socially and economically disadvantaged a person is, the more likely they are to suffer from these diseases. Diseases that are largely preventable. The spread of the virus has highlighted the needs of migrants, asylum seekers, and Roma people who already experience discrimination and health inequalities. They make up just some of the 26% of people in Europe living in overcrowded spaces. In confinement, people are more exposed to interpersonal violence at home – notably women and LGBTI people.
Mental Health
This social gradient also applies to risks of mental ill-health, which will be exacerbated by isolation, fear, and insecurity. A survey from the Netherlands National Institute for Public Health and the Environment found that more than a third of people say they felt much more anxious, despondent, stressed and lonely during the pandemic. About 20% are having more problems sleeping than before. In France, a survey from the public health institute found that 27% survey respondents reported a state of anxiety; the factors contributing to this feeling include being in an unstable financial position, having a poor understanding of transmission of the virus, feeling of being ill-equipped to adopt to recommended measures, and having little confidence in public authorities. People in deprived areas are less likely to receive treatment for mental ill-health 5In 2018, 26.2% of the European population with an income below 60 % of median equivalized income lived in overcrowded dwellings. Overcrowding rate by age, sex and poverty status – total population – EU-SILC survey 2018.
 Adapted from Baum, F. E.; More than the tip of the iceberg: health policies and research that go below the surface; https://doi.org/10.1136/jech.2009.091595
Adapted from Baum, F. E.; More than the tip of the iceberg: health policies and research that go below the surface; https://doi.org/10.1136/jech.2009.091595
What are the causes of health inequalities?

Complex and interlinked factors cause Health inequalities and the social gradient. They fundamentally result from socio-political factors that lead to differences in the distribution of power, money and resources between different population groups and social classes. These, in turn, result in differences in environmental and individual resources. Those resources are, for example, the quality and availability of employment, housing, transport, access to services, and social and cultural resources. Such resources are also referred to as determinants of health, because they affect opportunities for good health, and how people think, feel and act.
- the quality of care that an infant or child receives
- whether a person has sufficient income to meet their basic needs
- their employment status and conditions
- the quality of their housing and communities are all.
These factors affect whether individuals have the capacity, the opportunity or the motivation to, for example, eat well or to get adequate physical activity. They also determine if a person has access to quality treatment and care when illness occurs, and the ability to benefit from this.
5 contributing factors
WHO Europe has identified five conditions that contribute to health inequalities in self-reported health, mental health, and life satisfaction. The WHO Health Equity Status Report indicates that 90% of health inequalities can be explained by these 5 factors:
- Quality of health care.
- Financial insecurity.
- Poor quality housing and neighbourhood environment.
- Social exclusion.
- Lack of decent work and poor working conditions.
In recent years it has also become clear how levels of health inequalities are related to production and consumption patterns, particularly in highly industrialised economies like those in the EU. The destabilisation of the environment has grave repercussions for health and well-being. The effects of environmental degradation and climate change will ultimately affect the health and quality of life of everyone. However, they have a disproportionate effect on those who are already more vulnerable.