Social outcomes contracting (SOC), also known as outcome funds, is a novel mechanism for investment in health promoting services. SOCs are contracts in which payments are made only when pre-agreed social (or health-promoting) outcomes are achieved by the funded programme or organisation.
SOCs are different to a ‘payment-by-outputs’ approach and social impact bonds (SIBs). The most significant difference is the inclusion of the investor in the development stage. SOCs help participating organisations to align their incentives to achieve social outcomes, while also saving public expenditure due to their focus on prevention and generating return on investment.
The benefits of an outcome-based contract model come forth from its approach to public-service management that seeks to improve value and impact. Payment mechanisms can differ, as arrangements can include a proportion of upfront or activity-based payment that is not contingent on the achievement of a specified outcome. Some form of upfront payment or ‘fee-for-service’ has the potential to make the scheme more attractive to providers and investors. This is because the fee can be used to help start-up costs and reduces the risk they take on in agreeing to the contract.
Health Inequalities Impact Assessment (HIIA)
One tool that has potential to be used across financial approaches and health promoting services is a Health Inequalities Impact Assessment (HIIA). A HIIA is a tool to assess the impact on people of applying a proposed, new or revised policy or practice. HIIA assesses the impact on; health inequalities, people with protected characteristics, human rights, and socioeconomic circumstances. Many policies, plans, proposals or decisions have the potential to impact on health and potentially widen health inequalities. By conducting an HIIA the potential impacts can be considered and action taken to reduce those impacts.
Impact assessments help to:
- ensure non discrimination
- widen access to opportunities
- promote the interests of people with protected characteristics.
The HIIA should be conducted when the policy, plan or financial instrument is still in draft. It should be well enough developed to understand the potential impacts, but not so far developed that changes are not possible as a result of the assessment.
For an example of how social outcome contracting is used in Sweden to decrease sick leave and build health-promoting workplaces, watch this video and read the case study below.
Case study
In Sweden, a social outcomes contract project for a preventive and healthy workplace was developed in response to an increase in sick leave across the country. The costs of sick leave benefits had risen from 26.2 billion Swedish Krona in 2013 to 39.8 billion Swedish Krona in 2016 (+52%), a trend particularly noticeable in the workplaces of public regions and municipalities, compared to private employers. Increased sick leave imposed a high burden on these public employers, as they are responsible for covering the expenses of short-term sickness (1-14 days). In addition, a rise in sick leave increased indirect costs and negative effects, including productivity loss and lower quality in public services.
A pre-study conducted in Swedish municipalities, in collaboration between SALAR, RISE, the European Investment Bank and Kommuninvest, found that 20% of employees accounted for 75% of the costs of short-term sick leave. The identified risk group of employees were found to be absent on 3 or more occasions during a 12-month period. The pre-study further indicated that regions and municipalities did not put enough effort into early identification and intervention in terms of reducing sick leave and improving employee health.
The intervention
The project employs a multi-level approach to target both individual and organisational factors impacting occupational health. The health support enables early identification of ill-health and sick leave absence which, in combination with structural interventions (manager support), enables preventive and health promoting actions. Additionally, the interventions aim to generate long-term competence at the human relations department in terms of identification and implementation of preventive actions – thus establishing capacity for prevention in a broader perspective.
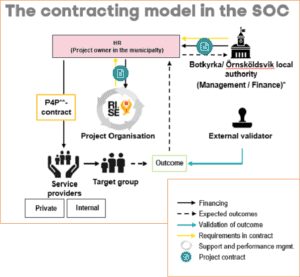
The structure of the SOC enables performance management and programme improvement, as well as collaboration between private and public sector organisations. The occupational health service provider is procured and contracted by the local authorities to perform services (health support and identification of risk groups). The public sector has played a big part in implementing the SOC, compared to other countries where SIBs have been adopted. Although the actors involved in a SOC or SIB may vary, the investors often include private actors. For instance, in the occupational health SOC in Botkyrka and Örnsköldsvik, the project is solely financed by the local authorities themselves, making it a unique example of a publicly-financed SOC. The project management organisation, consisting of a new entity formed by state-owned RISE and SALAR, assists with project monitoring, evaluation and support during the implementation process.
Financing specifics
The contractual partners in the SOC are the finance and human resources departments of the local authorities, as well as the intermediary organisation (RISE and SALAR). The total investments in the SOCs of two municipalities are 17,4 million Swedish Krona and 22,870 million Swedish Krona, respectively (€4 million in total) over a three-year period.
A financial instrument referred to as Sustainability Bond with Impact-Linked Return (SBIR) was designed to allow for institutional investors and a large investment volume (€100 million). The SBIR combines a loan (approx. 90%) with a social outcomes contract (approx. 10%) in order to achieve enough investment volume and a suitable risk profile. However, the Swedish local authorities decided to finance the SOC on their own.
During the procurement process of external service providers, various parameters were considered, including proposed risk-share agreements. The service providers were offered to bid on risk appetite - between 25% and 75% of reimbursement to be dependent upon the outcomes of the SOC. The contracted providers bid for 50% and 75% in each municipality. The financial commitments between the investors and service provider is regulated with a pay-for-performance contract based on this financial risk sharing with a potential premium for over-performing ,which is capped at half the risk level. Thus, there is financial risk sharing between the municipalities and the service providers.
Based on international experience, various case scenarios were outlined, defining the financial outcomes for all parties. All scenarios include a total intervention period of 36 months and a 9-month ramp-up to full intervention effect. Aiming for the low case scenario (12%) average reduction in net sick leave days will result in a break-even point. The expected base case scenario is on average 18% reduction, and the best case is 34% reduction of net short-term sick leave days. The estimated likelihood for achieving at least base case is 80%.
Measuring outcomes
As the results of health promoting interventions tend to only be observable years after the initial investments are made, it was challenging to identify long-term financing opportunities for a project aiming to prevent sick leave, particularly due to annual budget cycles.
The main outcome measurement used for financial evaluation is the direct costs for reduction in net short-term sick leave days (1-14 days), adjusted for national trends in sick leave. Other outcomes measured are long term sick leave (15+ days), purchasing of occupational health care services and size of risk group.
The share of repayment is dependent upon the financial risk of the service providers, but the cash flow also depends on the estimated cost for the service delivery per employee, the number of employees at the baseline measurement and the outcomes achieved. Evaluation is done by calculating the trend adjusted change of net sick leave days compared to the historic baseline. Reductions beyond break-even will result in repayments to the local authorities (66.25% and 81.6%) and to the service providers (33.75% and 18.4%). The cap on payments to the providers means that reductions above 150% of the investment value will go solely to the local authorities.
The ‘West London Zone’ area in London is home to around 66,000 children and young people aged 0-25 years. It is an area of deep inequality where 1 in 5 children and young people are not getting the support they need to thrive. Research indicates that around 12,000 children and young people in the area require additional support. Without it, they are more likely to face challenges later in life, including unemployment, social isolation, and poor mental and emotional health. However, the existing support systems often operate in isolation and lack the flexibly to address the specific needs of individual children.
Intervention and financing model
The West London Zone (WLZ) – recently renamed AllChild – is a targeted, early-action intervention that aims to connect West London’s rich ecology of local ‘social assets’ – including charities, nurseries, schools, community groups – to deliver better outcomes for children. The programme aims to ensure that children enter adulthood with good physical and mental health, are prepared for sustained employment, and can establish positive relationships.
The WLZ programme operates through a 2-year personalised support plan for each child, developed in collaboration with families, schools, and over 40 local partners. Each child is paired with a ''link worker'' who builds a trusted, lasting relationship with the child and ensures they receive the right support based on their personalised plan. The programme expanded its reach from working with 132 young people in 2016 to 1,001 in 2021.
To fund the project, WLZ uses a Collective Impact Bond. This funding model pools funding from local authorities, schools and private philanthropists, with additional contributions by central government and national lottery funding. Payments are only released when each individual child engages with the programme and makes measurable progress after two years, ensuring that even the most challenging cases are given the attention they need. There are seven ‘outcome areas’ that span across four domains: positive relationships, emotional and mental wellbeing, progress at school, and confidence and aspiration. Each outcome has specific measures which can release payment at the end of each child's two-year programme. While WLZ is paid on an outcomes-basis through the Collective Impact Bond, delivery partners are paid on a fee-for-service basis.
Key outcomes (if applicable) and associated measurements
In 2019, 71% of young people at risk in their peer relationships met their desired outcomes and 68% in 2020. In both 2019 and 2020, 64% of young people at risk concerning emotional wellbeing met their outcomes. In 2019, 51% of young people at risk in English courses and 33% at risk in mathematics courses achieved the desired outcomes.
Over the past 4 years, WLZ’s annual income tripled from £1.3m in 2016 to £3.9 million in the academic year 2019/20. The programme consistently achieved its Collective Impact Bond targets, which in turn has driven revenue generation. Philanthropy targets were also consistently surpassed.
However, it remains challenging to determine WLZ’s long-term impact once a child finishes the two-year programme. The COVID-19 pandemic also disrupted academic progress and emotional well-being, complicating data collection on the programme's overall impact.
Publications
The province of Noord-Brabant in the Netherlands faced challenges in scaling up social entrepreneurship initiatives that addressed societal issues but struggled with securing growth capital, fitting their intergrated approach within the compartmentalised government structures, and receiving sufficient appreciation for creating multiple social values. These challenges hindered the ability of social entrepreneurs to make a broader impact.
Intervention and financing model
To tackle these three key issues, the provincial government of Noord-Brabant launched The Brabant Outcomes Fund (BOF) in 2018. The fund focused on selecting social enterprises that could scale up their impact while contributing to multiple policy domains, particularly those aligned with the SDGs.
The provincial government cooperated with three impact investors and signed outcomes contracts with four entrepreneurs who work on addressing important societal problems in the region of Noord-Brabant in the Netherlands.
One specific example of a successful intervention under the BOF is "Stichting Sarban de Toekomst", which operates restaurants offering training and job opportunities to refugees facing challenges in accessing the labor market, contributing to SDG 8 (decent work for all) and SDG 10 (reduced inequalities). The business provided refugees with work experience and training, leading to over 80% of participants finding stable employment within six months. This intervention not only created jobs but also fostered social inclusion and empowerment.
Outcomes funds allow the funding of multiple SOC projects under one structure to accelerate growth, generate economies of scale and maximise learning.
Key outcomes (if applicable) and associated measurements
The emphasis in SOC is usually placed on outcomes that result in actual cost savings for the outcome payer. Such cost savings are relatively easy to measure objectively. However, in the BOF, cost saving was not the primary objective and outcomes that were not directly linked to savings were included as well. Consequently, other valuation methods were needed. In the BOF three different methods were used to determine the financial value of outcomes: 1) Cost-based pricing, 2) Valuation in accordance with market price and, 3) Valuation based on the opinion of the target group and/or stakeholders. If the agreed qualitative and quantitative results have been achieved, the provincial government will repay the working capital to the investors.
One specific example of a successful intervention under the BOF is Stichting Sarban de Toekomst, which operates restaurants offering training and job opportunities to refugees facing challenges in accessing the labor market. The business provided refugees with work experience and training, leading to over 80% of participants finding stable employment within six months. This intervention not only created jobs but also fostered social inclusion and empowerment, contributing to SDG 8 (decent work for all) and SDG 10 (reduced inequalities).
What made Brabant Outcomes Fund (BOF) unique compared to other Social Outcomes Contracting initiatives (SOC) is the way it included multiple values in the contracts. By this we mean that social values, such as empowerment and wellbeing, were an integral part of the contract alongside economic value.
In the first BOF, all 4 entrepreneurs achieved the agreed social results. Given this success, a second BOF initiative is being developed which aims for a total investment of 20 million euros through a combination of European, regional, public and private capital.